Almost
all of the calcium in the body (~99%) is found in the bones (and
teeth), where it is essential for building and maintaining bone to
give the bone its strength. The remaining ~1% is dissolved in the
bloodstream and other fluids where it is used for maintaining the
function of the heart, muscles, blood and nerves. We continuously
lose calcium each day through our skin, nails, sweat and urine.
What
happens if your diet is low in calcium?
Our
bodies cannot make calcium, therefore all our calcium requirements
are provided by our diet. If our diets do not provide sufficient
calcium, there will not be enough calcium available in the
bloodstream for our bodies to function properly. This means some of
the calcium crystals stored in the bone will dissolve to 'stock up'
the calcium needed in the bloodstream. If your calcium intake remains
too low, the calcium in your bone will continuously need to dissolve
and be released into your bloodstream, and you risk losing bone
strength.
Calcium
absorption
As
well as increasing your intake of calcium, it is also essential that
the calcium is able to be absorbed by the body. Calcium absorption
can be reduced by excessive alcohol or caffeine consumption, as well
as consuming a diet high in animal proteins or drinking soft drinks
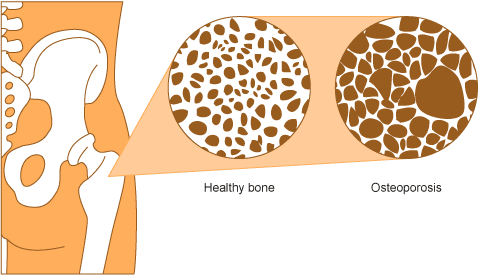
that contain phosphates. As we age, calcium is absorbed less
effectively from the intestine thus we need to increase our intake of
calcium to avoid losing bone density which may result in
osteoporosis.
The
greatest rate of bone growth is reached by puberty, and by age 30 we
reach our peak bone mass (maximum bone density). The higher our peak
bone mass, the better our bone health will be in the future. This is
particularly important for women as rapid bone loss occurs during the
menopause. As puberty is an essential time for determining your
overall bone health, it is critical that children and teenagers get
enough calcium.
Your
daily calcium
requirements depend on your age and sex. Less than half of
Australian adults get their daily recommended intake of calcium.
Sources
of calcium
Dairy
Dairy
foods such as milk, yoghurt and most cheeses are calcium-rich and
serve as the primary source of calcium in our diet. Calcium is also
more easily absorbed from dairy products compared to other food
groups.
Aim
to eat 2-3 serves a day such as a glass of milk, a slice of hard
cheese or a yoghurt.
 |
| Photo by adam morse on Unsplash |
Canned
fish
It's
not only humans that have high levels of calcium in their bones.
Consuming canned fish including the bones will also help you increase
your calcium intake.
Try
canned salmon or sardines!
Eat
more fruit and veg!
Small
amounts of calcium are also found in fruit and vegetables,
particularly greens such as broccoli and kale. Nuts are also a great
way to introduce more sources of calcium into your diet, particularly
almonds.
Useful
resources
Australian
dietary guidelines 2013
Nutrient
reference values for New Zealand and Australia
Arthritis
WA
Calcium
content of various foods
NHMRC
Food for Health